A 25yr old female came with chief complaints of SOB Grade II - III since 6 months
This is an online e log book to discuss our patient’s de- identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patient’s clinical problems with collective current best evidence based inputs. This e-log book reflects my patient centered online portfolio and your valuable inputs on the comments is welcome
Name :- P. Sai Krupa Sri (intern)
Roll no:- 113
Date :- 31/5/23
A 25yr old female came with chief complaints of SOB Grade II - III since 6 months
History of present illness :-
Patient was apparently asymptomatic until 2016 then developed headache, occipital region more, insidious in onset , gradually progressive, prominent with nausea and occasional vomitings, associated with photophobia, phonophobia, no lacrimation , no aggravating factors and relieved with medication.
She also had difficulty in writing ( associated with pain at tips ) and on investigation was found to have low hemoglobin (also had SOB, grade I - III ) jaundice and so, reports - Hb electrophoresis S/o HbE and mild iron deficiency anemia and was treated accordingly
In dec 2022 , patient had right hypochondric region pain , and on USG abdomen --> gallstones present and was operated for it.
Laproscopy cholecystectomy done.
In Feb 2022, patient experienced polyphagia, polydyspsia , nocturia present (3-4 times) and went for dental checkup , and on investigation , was found to have high sugars and was diagnosed to have diabetes, and since then she was on regular medication, presently using Tab.Lipoglobin HP BD and Tab. Vildamne 50 2 tabs (night).
Now SOB grade II - III increased since 6 months
Past history :-
Known case of diabetes mellitus since 1yr on medication Tab.Lipoglobin HP BD and Tab. Vildamne 50 2 tabs (night).
Not a known case of thyroid disorders , HTN , asthma
No chest pain and no orthopnea
Personal history:-
Diet- eggtarian
Appetite - decreased
Sleep - adequate
Bowel and bladder- regular
No allergies
Addiction - teetotaler
Tobacco - snuff
Family history:-
Grand father has diabetes mellitus II
Menstrual history:-
Aom- 13yrs
Menstrual cycle - 7/30-35days
General examination:-
Patient is conscious, coherent, co operative
Pallor present
No icterus, cyanosis, clubbing, lympadenopathy , edema
Vitals:-
Temp:- 98f
Pr- 96bpm
Rr- 16cpm
Bp- 120/80mm hg
Spo2- 96%
Grbs- 309 mg/dl
Systemic examination:-
Cvs- S1S2 heard , no murmurs
Rs- BAE present , NVBS present
P/A - soft , non tender
CNS- NAD








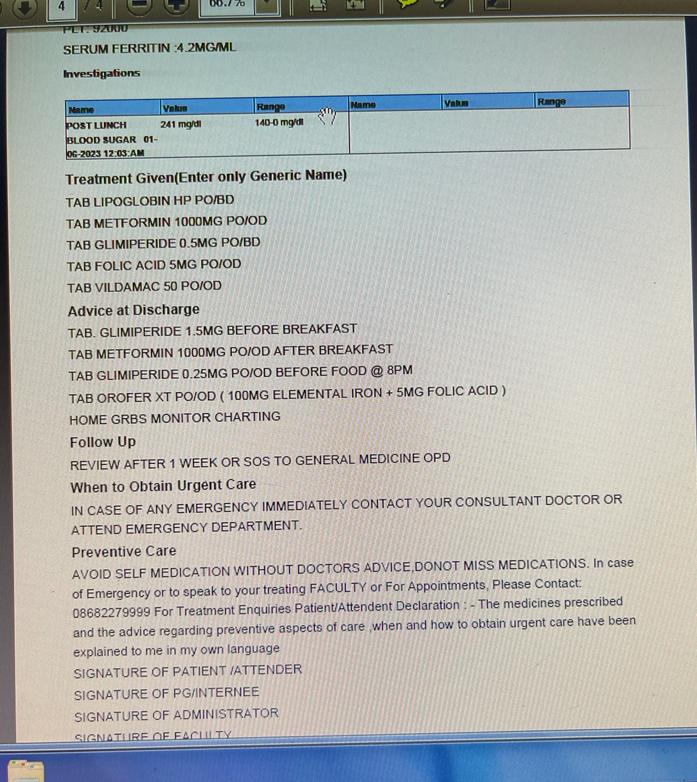
Investigation:-
FBS- 191mg/dl
PLBs:- 241mg/dl
HBA1C : 6.7
HEMOGLOBIN:- 6gm/dl
TLC- 7,800
PLT- 92,000
Provisional diagnosis:-
Metabolic syndrome with diabetes HbE thalassemia
Treatment:-
Tab.Lipoglobin HP BD
Tab. Vildamne 50
Tab. GLIMIPERIDE 0.5mg PO/BD
Tab. Metformin 1000mg PO/OD
Tab.folic acid 5mg PO/BD
Tab. Orofer XT PO/OD









Comments
Post a Comment